
Pediatric Sleep Apnea and Sleep Disordered Breathing in Children
ADHD in Children
ADHD is commonly misdiagnosed with Sleep Disordered breathing in children as both share similar symptoms.
Children with Sleep Disordered breathing frequently complain of morning headaches, are hyperactive during the day and avoid going to sleep until significantly tired. Often they tend to move their legs at night, sleep with mouth open, and even snore. In rare instances, breathing stops can be observed. These children are at risk of developing pediatric obstructive sleep apnea.
It is crucial to screen all children for signs of obstructed nasal breathing and take measures to prevent any breathing disturbances. It is our scope to provide comprehensive consultations for both children and adults seeking treatment for sleep disordered breathing and obstructive sleep apnea associated disorders.
Mouth Breathing and Obstructive Sleep Apne
Mouth breathing in children, especially when chronic, can have several negative effects on airway development, facial structure, and overall health. Here’s a detailed breakdown of how mouth breathing can impact the airway and related systems in kids:







Airway Development and Structure
- Narrowed airway: Chronic mouth breathing can alter the normal growth and development of the upper airway (nasal passages, pharynx, and even the lower airway), leading to a smaller, more constricted airway.
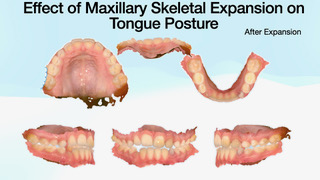
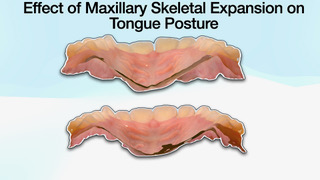
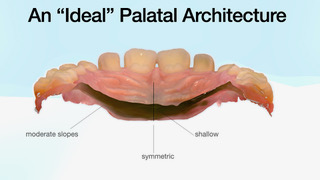
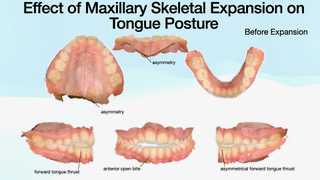
- High-arched palate: When kids breathe through their mouths, the tongue doesn’t rest against the palate as it normally would. This can lead to a narrow, high-arched palate, which reduces the width of the nasal airway.
- Underdeveloped maxilla and mandible: Lack of proper tongue posture due to mouth breathing can result in underdevelopment of the upper jaw (maxilla) and even the lower jaw (mandible), which further restricts airway space.
Increased Risk of Obstructive Sleep Apnea (OSA)
Mouth breathing is a significant risk factor for sleep-disordered breathing, including pediatric OSA. A constricted airway increases the chance of airway collapse during sleep, leading to disrupted sleep and poor oxygenation.
Poor Tongue Posture and Function
The tongue plays a critical role in shaping the oral cavity and maintaining airway patency. Mouth breathing causes low tongue posture, which contributes to:
- Improper orofacial development
- Reduced airway volume
- Functional issues with swallowing and speech
Facial and Dental Effects ("Adenoid Facies")
Chronic mouth breathing is associated with a distinctive facial appearance:
- Long, narrow face
- Open-mouth posture
- Droopy eyes, dark circles
- Small nostrils
- Dental malocclusions like overjet, crowding, and open bite
These changes are not just cosmetic—they correlate with a smaller, compromised airway.
Functional and Cognitive Issues
Poor oxygenation due to mouth breathing and disrupted sleep can lead to:
- Daytime fatigue
- Difficulty concentrating
- Behavioral issues
- Lower academic performance
- Some studies even link mouth breathing with symptoms that mimic ADHD
Common Causes of Mouth Breathing in Kids
- Chronic nasal congestion (from allergies, enlarged adenoids/tonsils, deviated septum)
- Habitual behavior
- Structural issues (e.g., tethered oral tissues like tongue tie)
Our Approach to Screening and Treatment of Sleep Disordered Breathing in Children
Our approach is focused on screening all children who present for the consultation in our practice for the signs of Sleep Disordered Breathing and Obstructive Sleep Apnea.
Treatment modalities include collaborative approach with pediatricians, ENT specialists, sleep physicians in developing the most effective sequence of interventions.
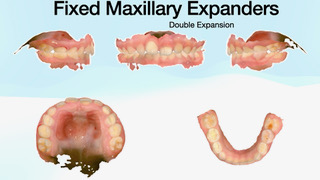
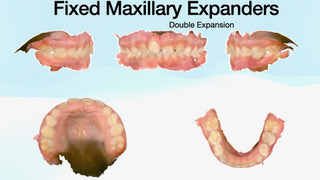
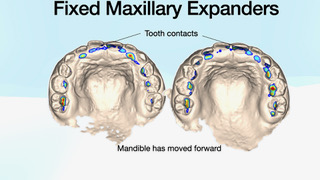
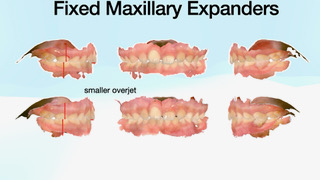
While in some cases children present with enlarged adenoids and tonsils which become the cause of obstruction of the upper airways and, thus, require intervention. In other cases, the amount of adenoid and tonsil enlargement is such that does not require immediate intervention (removal). Multiple studies and our clinical observations have proven that the amount of lymphoid tissue (adenoids and tonsils) may react to changes in the size and dimension of the upper airway in response to orthodontic treatment. Airway-focused orthodontic treatment in early childhood focuses on the development of the facial region that surrounds upper airways. Two main structures are mainly responsible for the development of the upper airway size and volume – the dimensions nad position of the maxilla (midface) and the position and relationship of the mandible relative to the maxilla and the face.
At Dr. Koval Orthodontics, our approach is focused on developing the face through bone growth. Bone growth is triggered via airway protocols of expansion and mandibular advancement.
